Fast Gas Analyzer for Bio-Physical Applications and Bioreactors
Based on the Oxigraf Model O2Cap Oxygen and CO2 analyzer, the O2Bio is specifically designed to provide gas monitoring of Bioreactor headspace and off-gas streams. The unit will measure continuously from an off-gas vent or periodically via a gas sample valve to take small 10-15ml samples from the bioreactor headspace via keypad or digital interface control.
The O2Bio integrates an Oxigraf tunable diode laser (TDL) oxygen sensor and a non-dispersive infrared (NDIR) CO2 sensor with a pump regulated gas sampling system. The analyzer features a bright vacuum fluorescent alphanumeric display (VFD), touch panel keypad, a rear 0-1VDC analog BNC output for O2 readings, rear terminal strip with limit detection relays and 4 – 20 mA analog outputs of O2 and CO2 reading, and a RS232 digital interface.
O2Bio – Bioreactor Off-Gas Monitoring of O2 and CO2
All inputs and outputs are CPC quick connect fittings with O-ring seals. Gas Inlet and Outlet with Swagelok or Luer fittings can be provided optionally.
The Oxigraf sensor uses laser diode absorption technology to measure oxygen concentration in the gas sample. A laser diode produces light in the visible spectrum at 760 nanometers. Light at this wavelength is absorbed by oxygen. To analyze oxygen the laser beam is focused through the sample gas onto a detector. Oxygen concentration is inversely proportional to the amount of light reaching the detector. An analysis is made every 10 ms.
The analyzer automatically zeroes at each measurement interval by electronically tuning the laser to oxygen non-absorption wavelength. CO2 is measured using a NDIR based accessory sensor and integrated into our hardware.
Oxygen measurements are made independent of sample pressure, gas temperature, and (in XC mode) other gases including Ar, He, H2, CO2 and H2O. Gases other than oxygen will not affect the measurement except for their dilution effect on the gas mixture.
APPLICATIONS:
Fast Gas Analysis of: Oxygen and CO2
Overlay and Sparge Gas Controller for Bioreactors
Microbial Systems & Biofuel Development
Biomass Growth Rate and Substrate Consumption Monitoring
Anaerobic Fermentation
Stem Cell & Mammalian Cell Cultures
Gas Sampling and Valve Control:
The O2Bio/O2Bio-B Analyzers are specifically designed to provide gas monitoring of Bioreactor headspace and off-gas streams. The unit will measure continuously from an off-gas vent or periodically via a gas sample valve to take small 10-15ml samples from the bioreactor headspace via keypad or digital interface control.
This Oxigraf analyzer is equipped with a solenoid sampling valve with 1 ms response time enabling sampling of very small sample volumes.
PERFORMANCE SPECIFICATIONS:
Range: 0 to 10% CO2; 5 to 100% Oxygen
Resolution: 0.1% in 0 to 100% O2 range; 0.01% in 0 to 10% CO2 range
Sample Flow: 50 to 250 ml/min pump on; 50 to 500 ml/min pump off.
Response Time: Approximately 150 ms @ 250 ml/min flow (depending on electronic filter setting).
Valve Response: 1 ms for Solenoid sampling valve
Stability (4hrs): ±0.2%.CO2 after 5 minute warm up; ±0.3%oxygen in XC mode, ±0.1% in oxygen LN mode
Dimensions: 7.5 x 3.0 x 14.0 inches (190 x 76 x 356 mm) WxHxD
Weight: 7 pounds (3.2 kg)
Warranty: One year
Back Panel Interface:
Back Panel O2Bio with rear terminal strip with limit detection relays:
The power on/off switch (Press “I” for on, “O” for off), 12 VDC power input jack, service interface, terminal block interface, and a gas outlet port are located on the instrument back panel. Power is supplied by an external 12 Volt, 2 Amp CSA Level 3 power supply. The RS – 232 port is provided to interface with a computer.
Calibration Kit:
Calibration Kit includes certified concentration gas cylinders, preset flow regulators, and tubing with connectors which mate with the analyzer and gas cylinder. The tubing assembly includes a fine flow needle valve. Instrumentation grade, certified calibration gas meets FDA standards for USP oxygen analyzers. Each cylinder provides approximately 3 months of daily calibrations. Calibration gas is shipped direct from the gas supplier.
In the relapsing remitting type of multiple sclerosis (MS) reducing relapses and neurodegeneration is crucial in halting the long-term impact of the disease. Medical disease-modifying treatments have proven effective, especially when introduced early in the disease course. However, patients still experience disease activity and disability progression, and therefore, supplemental early treatment strategies are warranted. Exercise appear to be one of the most promising supplemental treatment strategies, but a somewhat overlooked ‘window of opportunity’ exist early in the disease course. The objective of this study is to investigate exercise as a supplementary treatment strategy early in the disease course of MS.
Methods and analysis
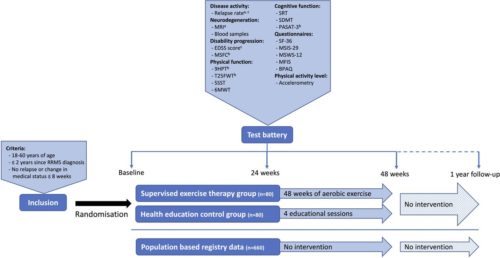
The presented Early Multiple Sclerosis Exercise Study is a 48-week (plus 1-year follow-up) national multicentre single-blinded parallel group randomised controlled trial comparing two groups receiving usual care plus supervised high-intense exercise or plus health education (active control). Additionally, data will be compared with a population-based control group receiving usual care only obtained from the Danish MS Registry. The primary outcomes are annual relapse rate and MRI derived global brain atrophy. The secondary outcomes are disability progression, physical and cognitive function, MS-related symptoms, and exploratory MRI outcomes. All analyses will be performed as intention to treat.
Figure 1 a: Primary outcome, b: Part of the Multiple Sclerosis Functional Composite, c: Outcomes available in the population based registry database.
Participants
Recruitment and eligibility
Patients with MS will be recruited via six Danish regional MS clinics (Aarhus University Hospital, Odense University Hospital, Clinics of Southern Denmark (Sønderborg, Esbjerg, Kolding), and Hospital Unit of Western Denmark), or via social media groups and events related to the Danish MS Society. In all cases, patients will be supplied with a leaflet explaining the rationale, design and content of the study and inviting them to participate. Those interested in participation will receive detailed written information as well as a leaflet from the National ethical committee explaining their rights as a participant in a health science research project. Furthermore, the project coordinator will contact participants by phone to explain the study, give the opportunity to ask questions, and to screen according to the inclusion criteria. Specifically, patients have to fulfil the following: (1) 18–60 years of age, (2) ≤2 years since clinical diagnosis with relapsing remitting MS and (3) no relapses or changes in medication ≤8 weeks prior to inclusion. Patients will be excluded if they: (1) are pregnant, or (2) have comorbidities or other issues thought to hinder participation in high intensity exercise activities. Finally, project nurses from the regional MS clinics confirm eligibility based on the patients’ medical records, and patients sign informed consent (standard formula from the Danish National Research Ethics Committee, see online supplemental material before inclusion.
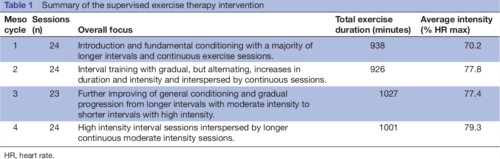
Table 1 Summary of the supervised exercise therapy intervention
Primary outcomes
The overall primary outcomes of the study are annual relapse rate and MRI-derived annual global brain atrophy rate.
Relapse rate
The number of relapses in the study period is obtained from the medical records of the included patients. This will be done in collaboration with the respective MS clinics, and all relapses will be confirmed by a neurologist. According to the Danish national neurological association, a relapse is defined as new symptoms or worsening of existing symptoms, causing neurological dysfunction for a minimum of 24 hours without any signs of infection or fever. This exacerbation must be preceded by a stable 4-week period. The annual relapse rate is calculated for each patient by dividing 365 days with the number of days in the study and multiplying by the number of relapses in the study period. Due to the clinically meaningful definition of this outcome any potential changes in the relapse rate will be considered clinically meaningful.
Secondary outcomes
Disability progression
Neurological impairments in MS can be assessed by grading the impairment of eight different functional systems (pyramidal, cerebellar, brain stem, sensory, bowel and bladder, visual, cerebral, other) to rate the total EDSS score. The EDSS score is considered the gold standard when assessing disability and disease progression in MS and it is used routinely as a clinical endpoint in trials of DMTs. In this study, the EDSS score will be determined for each participant by trained neurologists at the six collaborative MS clinics during routine clinical visits. Therefore, the EDSS score nearest to the date of inclusion, to the date of completion, and to the date of 1 year since completion will be used to assess the progression of disabilities. However, recent studies have pointed out limitations in the EDSS score such as insufficient inter-rater and intrarater reproducibility and a low responsiveness—especially at the lower end of the scale. Therefore, the main measure of disability progression will be the Multiple Sclerosis Functional Composite (MSFC).
Inflammatory and neurodegenerative biomarkers
Blood samples will be collected in resting state at baseline, after 24 weeks, after 48 weeks, and again at 1-year follow-up. Patients will be allowed a minimum of 5 min supine rest before blood collection from the antecubital vein. Blood samples will be collected in ethylenediaminetetraacetic acid-treated tubes, resting for 90 min, and subsequently centrifuged at 1200 g for 10 min. Thereafter serum will be extracted and divided into five aliquots and stored at −80°C until further analyses.
Analysis of blood samples will be exploratory and aim to investigate the effects of exercise on relevant biomarkers, such as Glial Fibrillar Acid Protein, proinflammatory and anti-inflammatory markers (eg, interleukin-6, interleukin-10, interleukin-17, tumour necrosis factor-α) as well as neurodegenerative (eg, neurofilament light chain) and neurotrophic markers (eg, brain-derived neurotrophic factor, insulin-like growth factor).
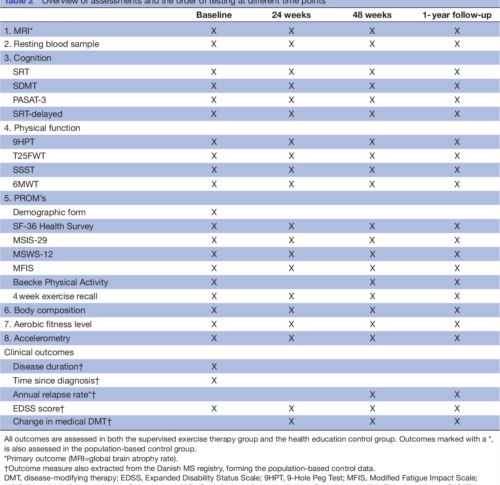
Table 2 Overview of assessments and the order of testing at different time points
DISCUSSION AND PERSPECTIVES
The presented study seeks to investigate supervised exercise as a supplemental treatment strategy early in the disease course of relapsing remitting MS. Effects of the
intervention will primarily be investigated on measures of disease activity and neurodegeneration, and secondarily on measures of disability progression, cognitive and physical function, and symptoms of fatigue. Efforts investigating the effects of exercise beyond rehabilitation (eg, as a supplemental disease-modifying strategy) are warranted and an overlooked ‘window of opportunity’ early in the disease course for MS exercise therapy have previously been identified. Importantly, the present study addresses both of these issues making the approach novel and innovative. Furthermore, the present study complies with the recommendations from
recent publications guiding the field of MS rehabilitation and exercise aligning the methodology with the current stage of the literature. Specifically, the study has
clearly defined primary outcomes and sample size calculations based hereupon (resulting in a large-scale exercise study), includes a rather long-term supervised exercise intervention and a well-monitored active control group (eg, importantly controlling the physical activity level of participants).
In summary, this is the first-ever study to investigate the effects of exercise in the very early stages of MS and thereby taking a more preventive approach aiming at lowering the disease activity more than medical DMTs alone aiming at maintaining (or even improving) functional and neurological reserve capacity. We expect the present study to hold the potential to change the current clinical practice regarding exercise therapy with MS. In particular, the present study may provide the first data supporting a warranted shift of paradigm where exercise will be considered a supplemental treatment strategy from an early timepoint in the disease course of MS. If these early exercise efforts show additional disease-modifying and neuroprotective effects, this is inherently of major interest to the individual MS patient, yet also to the healthcare system. While medical DMTs constitute the majority of healthcare costs for patients with mild MS early exercise efforts
may be a cost-effective supplemental treatment strategy to minimise disability progression and the huge-related costs. Another highly important perspective of early
exercise efforts as a supplemental treatment strategy in MS is the improvement of general health of the patients and the derived reduction in the increased risk of lifestyle-related comorbidities observed in patients with MS.
Authors: Morten Riemenschneider1, Lars G Hvid1, Steffen Ringgaard2, Mikkel K E Nygaard3, Simon F Eskildsen3, Thor Petersen4, Egon Stenager5,6, Ulrik Dalgas1
1 Exercise Biology, Department of Public Health, Aarhus University, Aarhus, Denmark 2 Exercise Biology, Department of Public Health, Aarhus University, Aarhus, Denmark.
3 The MR Research Centre, Aarhus University Hospital, Aarhus N, Denmark.
4 Center of Functionally Integrative Neuroscience, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark.
5 The Multiple Sclerosis Clinic, Department of Neurology, Aarhus University Hospital, Aarhus, Denmark.
6 Institute of Regional Health Research, University of Southern Denmark, Odense, Denmark.
Published in: BMJ Open, 11 Jan 2021, 11(1):e043699
Background: Oxygen is an essential therapy for hypoxemia but is scarce in low-income settings. Oxygen conserving devices optimize delivery, but to date have been designed for adults in high-income settings. Here we present the development and clinical pilot study of an oxygen-sparing nasal reservoir cannula (OSNRC) for pediatric use in low-income settings.
Methods
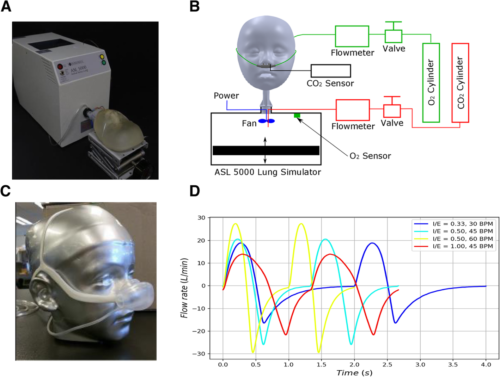
(1) Pre-clinical development of a novel OSNRC using a simulated respiratory circuit with metabolic simulator and anatomically accurate face-airway models. Simulated breathing waveforms were designed based on airway resistance, lung compliance, respiratory rate, and tidal volume of spontaneous breathing for three disease conditions.
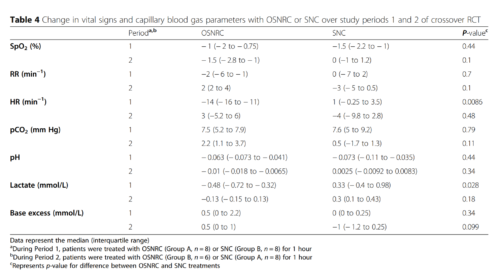
(2) Pilot, randomized, controlled, non-blinded, cross-over study of the OSNRC vs standard nasal cannula (SNC) among children hospitalized with hypoxemic pneumonia in Uganda. Eight children were randomized to OSNRC followed by SNC, and eight were randomized to SNC followed by OSNRC.
Results
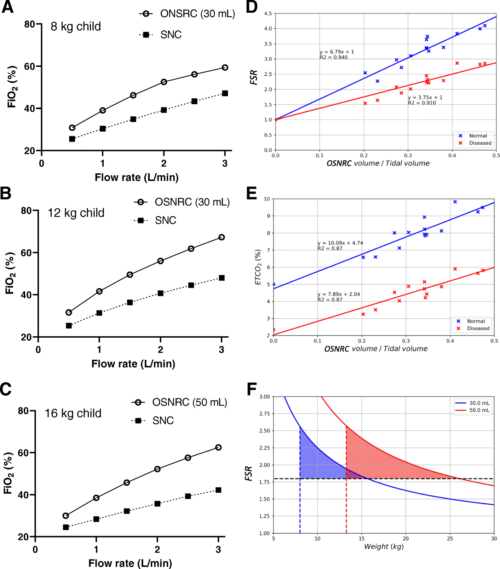
The laboratory simulation showed that the OSNRC provided the same or higher fraction of inspired oxygen at approximately 2.5-times lower flow rate compared to SNC. The flow savings ratio exhibited a linear relationship with the OSNRC volume to tidal volume ratio with a slope that varied with breathing waveforms. The range of performance from different breathing waveforms defined a performance envelope of the OSNRC. Two mask sizes (30 mL and 50 mL) provided sufficient coverage for patients between the 3rd and 97th percentile in our targeted age range. In the clinical pilot study, the rise in capillary blood pCO2 was similar in the OSNRC and SNC groups, suggesting that the OSNRC was not associated with CO2 retention. There were no significant differences between OSNRC and SNC with respect to clinical adverse events, lactate levels, pH, and SpO2. The OSNRC group had a higher mean SpO2 than the SNC group (adjusted mean difference, 1.4, 95% confidence interval 1.1 to 1.8), showing oxygen delivery enhancement.
Conclusion
The OSNRC enhances oxygen delivery without causing CO2 retention and appears to be well-tolerated by pediatric patients. If safety, efficacy and tolerability are confirmed in larger trials, this device has the potential to optimize oxygen delivery in children in low-resource settings, reducing the global burden of pediatric pneumonia.
Authors: Jerry Mulond1 , Stella Maleni1, Hellen Aanyu-Tukamuhebwa2, Ezekiel Mupere2,3, Alfred Onubia Andama4, Chin Hei Ng5, Stephen Burkot5, Ella M. E. Forgie6, Qaasim Mian6, Christine M. Bachman5, Gerard Rummery7, Daniel Lieberman5, David Bell5,8, Michael T. Hawkes6,9,10,11,12*† and Akos Somoskovi5†
1 Infectious Diseases Research Collaboration, Kampala, Uganda.
2 Department of Pediatrics and Child Health, Mulago National Referral Hospital and Makerere University, Kampala, Uganda.
3 Department of Pediatrics, Makerere, University College of Health Sciences, Kampala, Uganda.
4 Department of Medicine, Makerere University College of Health Sciences, Kampala, Uganda.
5 Intellectual Ventures, Global Good Fund, Bellevue, WA, USA.
6 Department of Pediatrics, University of Alberta, 3-588D Edmonton Clinic Health Academy, 11405 87 Ave NW, Edmonton, Alberta T6G 1C9, Canada.
7 ResMed Ltd., Bella Vista, Australia.
8 Present address: Issaquah, USA.
9 Department of Medical Microbiology and Immunology, University of Alberta, Edmonton, Canada.
10 School of Public Health, University of Alberta, Edmonton, Canada.
11 Stollery Science Lab, Edmonton, Canada.
12 Women and Children’s Health Research Institute, Edmonton, Canada
* Correspondence: mthawkes@ualberta.ca †
Michael T. Hawkes and Akos Somoskovi contributed equally to this work
Oxigraf is proud of supporting the Thornhill Medical COVID-19 Response Action Plan!
Thornhill Medical is answering the call to support the fight against COVID-19, producing and delivering the MOVES® SLC™ devices to help save lives across the country. Combining an O₂ concentrator, ventilator, suction & vital signs monitoring in a rugged battery-powered portable unit, MOVES® SLC™ is a proven, mobile integrated life support technology. It’s Canadian advanced innovation at its best.
Oxigraf is now part of the Made in California Program, California’s trusted resource for a thriving manufacturing industry. Made in California is dedicated to highlighting the contributions of California’s manufacturers and raising awareness of the products made in the Golden State. Oxigraf is proud of contributing to the success of keeping manufacturing in California.
CMTC is affiliated with the National Institute of Standards and Technology (NIST) and is part of the Hollings Manufacturing Extension Partnership (MEP) Program. The MEP Program is an outgrowth of the U.S. Government policy to develop and deploy technology, management, and technical expertise for improving the competitiveness of manufacturing for small and medium-sized companies.
A SpaceX Falcon 9 rocket carrying the company’s Crew Dragon spacecraft is launched on NASA’s SpaceX Crew-1 mission to the International Space Station on Sunday, Nov. 15, 2020, at NASA’s Kennedy Space Center in Florida. Credits: NASA/Joel Kowsky
An international crew of astronauts is en route to the International Space Station following a successful launch on the first NASA-certified commercial human spacecraft system in history. NASA’s SpaceX Crew-1 mission lifted off at 7:27 p.m. EST Sunday from Launch Complex 39A at the agency’s Kennedy Space Center in Florida.
The SpaceX Falcon 9 rocket propelled the Crew Dragon spacecraft with NASA astronauts Michael Hopkins, Victor Glover, and Shannon Walker, along with Soichi Noguchi of the Japan Aerospace Exploration Agency (JAXA), into orbit to begin a six-month science mission aboard the space station.
“NASA is delivering on its commitment to the American people and our international partners to provide safe, reliable, and cost-effective missions to the International Space Station using American private industry,” said NASA Administrator Jim Bridenstine. “This is an important mission for NASA, SpaceX and our partners at JAXA, and we look forward to watching this crew arrive at station to carry on our partnership for all of humanity.”
The Crew Dragon spacecraft, named Resilience, will dock autonomously to the forward port of the station’s Harmony module about 11 p.m. Monday, Nov. 16. NASA Television and the agency’s website are providing ongoing live coverage through docking, hatch opening, and the ceremony to welcome the crew aboard the orbiting laboratory.
“I could not be more proud of the work we’ve done here today,” said Gwynne Shotwell, president and chief operating officer of SpaceX. “Falcon 9 looked great, Dragon was dropped off into a beautiful orbit about 12 minutes into the mission, and we’ll get more data as we go.”
NASA & SpaceX – Dragon Crew-1 Mission patch (Credit: NASA)
The Crew-1 mission is the first of six crewed missions NASA and SpaceX will fly as part of the agency’s Commercial Crew Program. This mission has several firsts, including:
The first flight of the NASA-certified commercial system designed for crew transportation, which moves the system from development into regular flights;
The first international crew of four to launch on an American commercial spacecraft;
The first time the space station’s long duration expedition crew size will increase from six to seven crew members, which will add to the crew time available for research; and
The first time the Federal Aviation Administration has licensed a human orbital spaceflight launch. The astronauts named the Crew Dragon spacecraft Resilience, highlighting the dedication teams involved with the mission have displayed and to demonstrate that when we work together, there is no limit to what we can achieve. They named it in honor of their families, colleagues, and fellow citizens.
“Watching this mission launch is a special moment for NASA and our SpaceX team,” said Steve Stich, manager of NASA’s Commercial Crew Program. “We are looking forward to getting this crew to station to continue our important work, and I want to thank the teams for the amazing effort to make the next generation of human space transportation possible.”
During flight, SpaceX commands the spacecraft from its mission control center in Hawthorne, California, and NASA teams monitor space station operations throughout the flight from the Mission Control Center at the agency’s Johnson Space Center in Houston.
Hopkins, Glover, Walker, and Noguchi will join the Expedition 64 crew of Commander Sergey Ryzhikov and Flight Engineer Sergey Kud-Sverchkov, both of the Russian space agency Roscosmos, and Flight Engineer Kate Rubins of NASA.
“It is an honor to have our Japanese astronaut launch on this Crew-1 Dragon as the first astronaut of the International Partner participating in the ISS program,” said Hiroshi Sasaki, JAXA vice president. “We look forward to having him conduct lots of science and demonstrate the technology, for here on Earth and for the future. I would also like to thank NASA and SpaceX for their tremendous effort to make this happen.”
Rubins, Hopkins, Glover, Walker, and Noguchi will participate in a live crew news conference from orbit at 9:55 a.m. Thursday, Nov. 19, on NASA TV and the agency’s website.
Crew-1 Astronauts
SpaceX’s Crew-1 mission for NASA will fly (from left) astronauts Mike Hopkins, Soichi Noguchi, Shannon Walker, and Victor Glover to orbit aboard a Crew Dragon spaceship. Credit: NASA
Michael Hopkins is commander of the Crew Dragon spacecraft and the Crew-1 mission. Hopkins is responsible for all phases of flight, from launch to re-entry. He also will serve as an Expedition 64 flight engineer aboard the station. Selected as a NASA astronaut in 2009, Hopkins spent 166 days in space as a long-duration crew member of Expeditions 37 and 38 and completed two spacewalks totaling 12 hours and 58 minutes. Born in Lebanon, Missouri, Hopkins grew up on a farm outside Richland, Missouri. He has a bachelor’s degree in aerospace engineering from the University of Illinois, and a master’s degree in aerospace engineering from Stanford University. Before joining NASA, Hopkins was a flight test engineer with the U.S. Air Force. Follow Hopkins on Twitter.
Victor Glover is the pilot of the Crew Dragon spacecraft and second-in-command for the mission. Glover is responsible for spacecraft systems and performance. He also will be a long-duration space station crew member. Selected as an astronaut in 2013, this is his first spaceflight.
The California native holds a Bachelor of Science degree in general engineering from California Polytechnic State University, a Master of Science degree in flight test engineering and a master’s degree military operational art and science from Air University, and a Master of Science degree in systems engineering from Naval Postgraduate School. Glover is a naval aviator and was a test pilot in the F/A‐18 Hornet, Super Hornet, and EA‐18G Growler aircraft. Follow Glover on Twitter and Instagram.
Shannon Walker is a mission specialist for Crew-1. As a mission specialist, she works closely with the commander and pilot to monitor the vehicle during the dynamic launch and re-entry phases of flight. She also is responsible for monitoring timelines, telemetry, and consumables. Once aboard the station, Walker will become a flight engineer for Expedition 64. Selected as a NASA astronaut in 2004, Walker launched to the International Space Station aboard the Russian Soyuz TMA-19 spacecraft as the co-pilot, and spent 161 days aboard the orbiting laboratory. More than 130 microgravity experiments were conducted during her stay in areas such as human research, biology, and materials science. A Houston native, Walker received a Bachelor of Arts degree in physics from Rice University, as well as a Master of Science degree and a doctorate in space physics, both from Rice University, in 1992 and 1993, respectively.
Soichi Noguchi also is a mission specialist for Crew-1, working with the commander and pilot to monitor the vehicle during the dynamic launch and re-entry phases of flight, and keeping watch on timelines, telemetry and consumables. Noguchi also will become a long-duration crew member aboard the space station. He was selected as an astronaut candidate by the National Space Development Agency of Japan (NASDA, currently the Japan Aerospace Exploration Agency) in May 1996. Noguchi is a veteran of two spaceflights. During STS-114 in 2005, Noguchi became the first Japanese astronaut to perform a spacewalk outside the space station. He performed a total of three spacewalks during the mission, accumulating 20 hours and 5 minutes of spacewalking time. He launched aboard a Soyuz spacecraft in 2009, to return to the station as a long-duration crew member. The Crew Dragon will be the third spacecraft Noguchi has flown to the orbiting laboratory. Follow Noguchi on Twitter and Instagram.
Mission Objectives
The Crew-1 astronauts’ zero-g indicator, “The Child” (“Baby Yoda”) from the Disney+ Star Wars series “The Mandalorian” floats into pilot Victor Glover’s seat on the SpaceX Crew Dragon. (NASA TV)
The crew will conduct science and maintenance during a six-month stay aboard the orbiting laboratory and will return in spring 2021. It is scheduled to be the longest human space mission launched from the United States. The Crew Dragon spacecraft is capable of staying in orbit for at least 210 days, as a NASA requirement.
Crew Dragon also is delivering more than 500 pounds of cargo, new science hardware and experiments inside, including Food Physiology, a study of the effects of an optimized diet on crew health and, Genes in Space-7, a student-designed experiment that aims to better understand how spaceflight affects brain function, enabling scientists to keep astronauts healthy as they prepare for long-duration missions in low-Earth orbit and beyond.
Among the science and research investigations the crew will support during its six-month mission are a study using chips with tissue that mimics the structure and function of human organs to understand the role of microgravity on human health and diseases and translate those findings to improve human health on Earth, growing radishes in different types of light and soils as part of ongoing efforts to produce food in space, and testing a new system to remove heat from NASA’s next generation spacesuit, the Exploration Extravehicular Mobility Unit (xEMU).
During their stay on the orbiting laboratory, Crew-1 astronauts expect to see a range of uncrewed spacecraft including the next generation of SpaceX cargo Dragon spacecraft, the Northrop Grumman Cygnus, and the Boeing CST-100 Starliner on its uncrewed flight test to the station. They also will conduct a variety of spacewalks and welcome crews of the Russian Soyuz vehicle and the next SpaceX Crew Dragon in 2021.
At the conclusion of the mission, the Crew-1 astronauts will board Crew Dragon, which will then autonomously undock, depart the space station, and re-enter Earth’s atmosphere. Crew Dragon also will return to Earth important and time-sensitive research. NASA and SpaceX are capable of supporting seven splashdown sites located off Florida’s east coast and in the Gulf of Mexico. Upon splashdown, the SpaceX recovery ship will pick up the crew and return to shore.
NASA’s Commercial Crew Program is delivering on its goal of safe, reliable, and cost-effective transportation to and from the International Space Station from the United States through a partnership with American private industry. This partnership is changing the arc of human spaceflight history by opening access to low-Earth orbit and the International Space Station to more people, more science, and more commercial opportunities.
The space station remains the springboard to NASA’s next great leap in space exploration, including future missions to the Moon and, eventually, to Mars. For more than 20 years, humans have lived and worked continuously aboard the International Space Station, advancing scientific knowledge and demonstrating new technologies, making research breakthroughs not possible on Earth. As a global endeavor, 242 people from 19 countries have visited the unique microgravity laboratory that has hosted more than 3,000 research and educational investigations from researchers in 108 countries and areas.
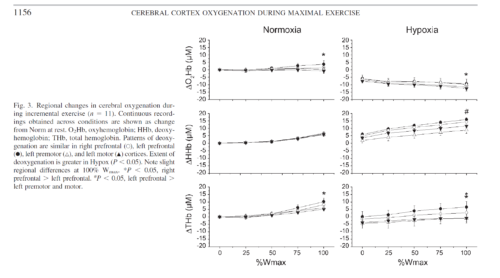
Reductions in prefrontal oxygenation near maximal exertion may limit exercise performance by impairing executive functions that influence the decision to stop exercising; however, whether deoxygenation also occurs in motor regions that more directly affect central motor drive is unknown. Multichannel near-infrared spectroscopy was used to compare changes in prefrontal, premotor, and motor cortices during exhaustive exercise. Twenty-three subjects performed two sequential, incremental cycle tests (25 W/min ramp) during acute hypoxia [79 Torr inspired Po(2) (Pi(O(2)))] and normoxia (117 Torr Pi(O(2))) in an environmental chamber. Test order was balanced, and subjects were blinded to chamber pressure. In normoxia, bilateral prefrontal oxygenation was maintained during low- and moderate-intensity exercise but dropped 9.0 +/- 10.7% (mean +/- SD, P < 0.05) before exhaustion (maximal power = 305 +/- 52 W). The pattern and magnitude of deoxygenation were similar in prefrontal, premotor, and motor regions (R(2) > 0.94). In hypoxia, prefrontal oxygenation was reduced 11.1 +/- 14.3% at rest (P < 0.01) and fell another 26.5 +/- 19.5% (P < 0.01) at exhaustion (maximal power = 256 +/- 38 W, P < 0.01). Correlations between regions were high (R(2) > 0.61), but deoxygenation was greater in prefrontal than premotor and motor regions (P < 0.05). Prefrontal, premotor, and motor cortex deoxygenation during high-intensity exercise may contribute to an integrative decision to stop exercise. The accelerated rate of cortical deoxygenation in hypoxia may hasten this effect.
Methods
Subjects.
After approval from the Colorado Multiple Institutional Review Board, 25 active, healthy volunteers (23 men and 2 women) from the Denver, CO, metropolitan area (elevation 1,650 m) provided written, informed consent to participate in a larger study investigating the etiology of acute mountain sickness. Physical examinations, including blood and urine tests, were conducted to verify general health before participation. All study procedures followed ethical guidelines established by the Declaration of Helsinki.
Study design.
Two incremental exercise tests were performed in an environmental chamber under ambient normobaric [normoxic (Norm), 610 Torr barometric pressure (Pb), 118 Torr inspired Po2 (PiO2)] and hypobaric [hypoxic (Hypox), 425 Torr Pb, 79 Torr PiO2] conditions to assess aerobic fitness for the larger study. Both tests were performed during a single chamber session to allow direct comparisons between Norm and Hypox without introduction of error from sensor placement/replacement. Tests were counterbalanced to control for order using a blinding strategy that varied chamber pressure to elicit similar sounds and changes in ear pressure during standardized 15-min ascent and descent periods. After arrival at the target Pb, 15 min were needed to adjust the cycle ergometer (Velotron Dynafit Pro, Racermate, Seattle, WA) and equip subjects with instrumental sensors (see below). Resting data were collected for 2 min before a 5-min warm-up at 50 W. Work rate was then incrementally increased using a 25 W/min ramp protocol to exhaustion. Subjects were blinded to elapsed time, power output, pedal revolutions per minute, and all physiological signals. Cool-down exercise was performed at 50 W for 5 min before chamber pressure was adjusted. After 15 min of ascent/decent and 15 min of rest at the second Pb, the protocol was repeated.
Results
Subjects.
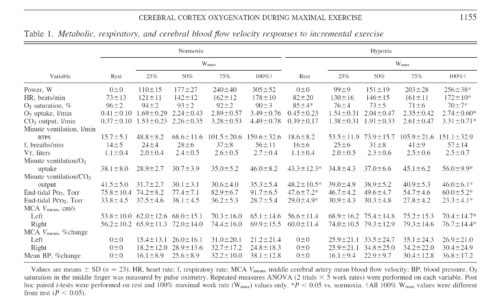
Twenty-three subjects (29 ± 8 yr of age, 73.7 ± 10.0 kg body wt, 181.7 ± 8.0 cm) completed both trials. Two subjects (with NIRS configuration 1) completed the Norm trial but were excluded from further study because of nausea and/or paresthesia during the subsequent depressurization period. Metabolic and power responses to both conditions were representative of physically fit, age-matched individuals (Table 1). Hypox reduced maximal V̇o2 and Wmax by 16 ± 6% and 21 ± 12%, respectively (P < 0.01). Order of trials did not affect the difference in maximal V̇o2 (P = 0.20) or Wmax (P = 0.95) between conditions, and 8 of 23 subjects were unable to retrospectively identify the order of testing.
Conclusions.
Cortical deoxygenation during high-intensity exercise is not restricted to prefrontal regions of the brain. Deoxygenation in premotor and motor cortices may contribute to fatigue and/or decisions to stop exercising. Acute hypoxia exacerbates cortical deoxygenation and, thus, may hasten these effects. Future functional NIRS studies are needed to expand our understanding of the role of cerebral activity in exhaustive whole body exercise.
Authors: Andrew W. Subudhi, Brittany R. Miramon, Matthew E. Granger, and Robert C. Roach
University of Colorado Altitude Research Center, Denver and Colorado Springs Campuses, Colorado Springs